Turnout: the hidden risks of chasing more rotation
A high-quality turnout is not the one that seeks the greatest possible range of motion, but rather the one that can generate rotation from the hip and maintain it with control, stability and safety.
The pursuit of “180 degrees” is part of the aesthetic of classical ballet. But does more rotation always mean better technique?
The en-dehors — or turnout — is one of the most distinctive characteristics of classical dance. The ability to perform movements with the lower limbs in external rotation allows dancers to execute specific positions and movements, contributing to aesthetics, range of motion and artistic expression.
However, there is a fundamental difference between having available rotation and forcing a position that the body cannot control.
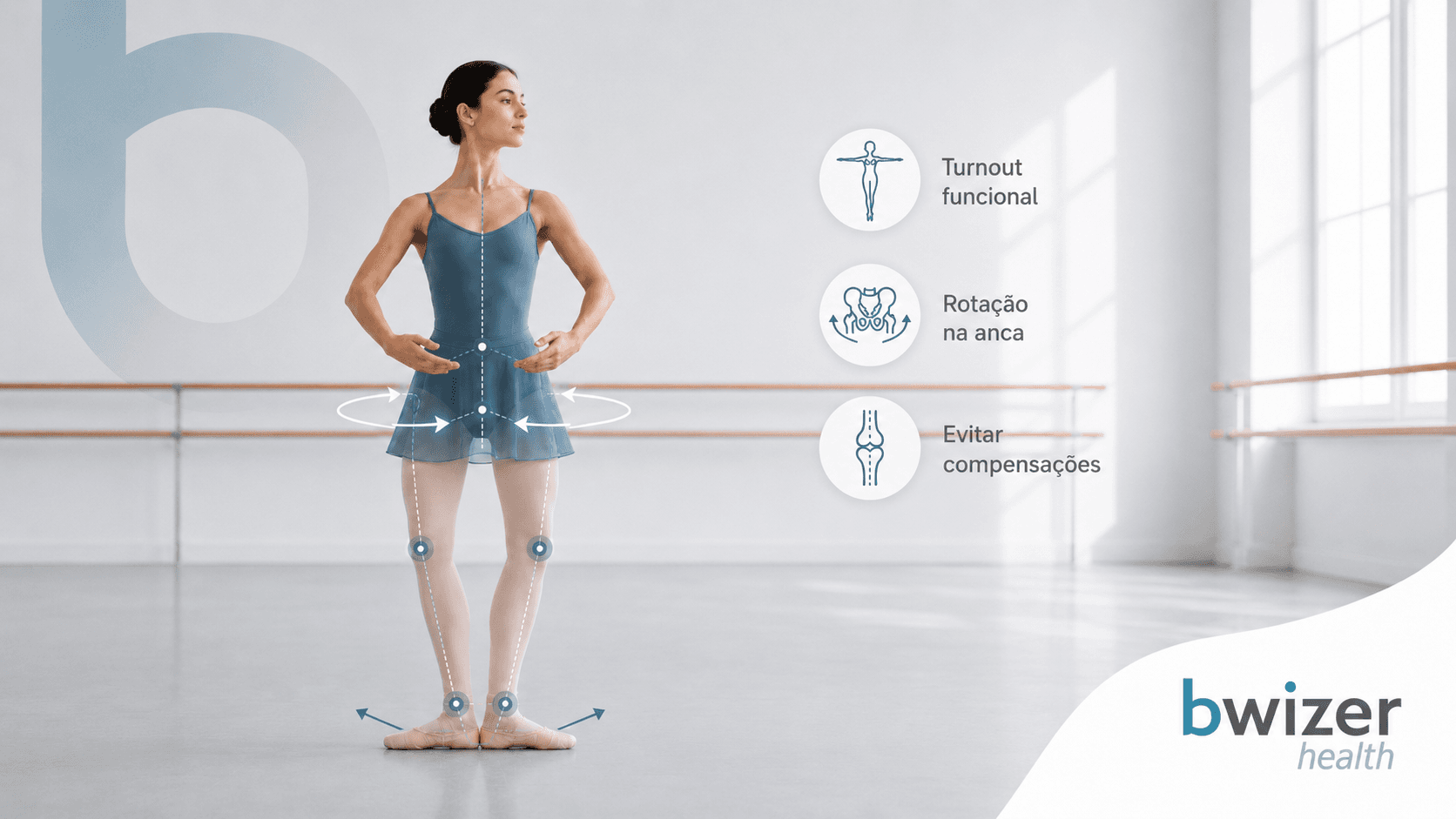
When the pursuit of turnout exceeds the functional capacity of the structures involved, the body begins to find alternative ways to compensate for this lack of rotation. These compensations may increase stress on the knee, ankle and foot, contributing to the development of pain and overuse injuries.
In dance, where the same movement patterns are repeated thousands of times, small biomechanical changes can become significant over time.
Functional turnout vs forced turnout: what is the difference?
Not all turnout is the same.
Functional turnout: rotation with control
Functional turnout occurs when external rotation is produced mainly through the hip joint, through the coordinated action of the muscles responsible for hip rotation and stabilisation.
In this case:
- the pelvis remains stable;
- the knee follows the direction of the toes;
- the foot maintains a balanced base of support;
- the muscles are able to control the position throughout movement.
The available range can vary significantly between dancers. Quality turnout does not depend only on the number of degrees achieved, but on the ability to produce and control that rotation during movements such as pliés, relevés, jumps or adages.
Forced turnout: when the body seeks rotation where it does not exist
Forced turnout occurs when a dancer attempts to achieve greater foot opening without having the same capacity for hip external rotation.
To achieve this position, the body may rely on compensations in other areas:
- tibial rotation;
- changes in knee alignment;
- excessive adaptation of the foot;
- alterations in pelvic and lumbar spine position.
The visual result may resemble the desired aesthetic, but the movement is no longer performed in a controlled position.
According to clinical literature, turnout assessment should specifically distinguish between active available rotation and rotation achieved through compensations from the knee and foot.
The role of the hip: where turnout truly begins
The hip joint plays a central role in turnout because it is primarily responsible for external rotation of the lower limb.
The ability to externally rotate depends on several factors:
- individual joint anatomy;
- available mobility;
- strength of the external rotator muscles;
- neuromuscular control.
There is no single ideal rotation value that applies to every dancer. Each person’s anatomy influences their naturally available range of motion.
When the hip cannot provide the required rotation, other joints begin to take on this movement.
This is where compensations appear.
When the knee starts compensating
The knee is a joint primarily designed for flexion and extension. Although it allows some rotation, it should not be used as the main source of turnout.
When a dancer forces external rotation below the hip, a combination of factors may occur:
- excessive tibial torsion;
- changes in the alignment between hip, knee and foot;
- increased rotational stress on joint structures.
A common sign of compensation is when the knee does not follow the direction of the second toe during movements such as the plié.
This alteration may increase shear forces within the joint and contribute to issues such as anterior knee pain or lower limb alignment dysfunctions.
The foot also plays a role
The foot is the point of contact with the floor and plays an essential role in dancer stability.
When there is an attempt to artificially increase turnout, strategies such as the following may appear:
- collapse of the medial arch;
- excessive pronation;
- inadequate weight distribution;
- “gripping” the floor with the toes to create stability.
These strategies may temporarily allow the dancer to maintain an aesthetic position, but they increase the demands placed on distal structures such as the ankle and foot.
The ankle-foot complex is one of the regions frequently affected by dance-related injuries due to the combination of repetitive loading, extreme positions and high technical demands.
How can you tell if your turnout is being compensated?
Some signs may indicate that rotation is being achieved through less efficient strategies:
1. The foot rotates more than the hip allows
When the feet show a large degree of external rotation, but the pelvis and hip do not follow the movement, distal compensation may be occurring.
2. The knee and foot lose alignment
During a plié, the knee should follow the direction of the toes. If the foot rotates outward while the knee remains facing forward, alignment is compromised.
3. There is a need to “grip” the floor
Toe gripping may be a strategy used for stability when proximal control or lower limb stability is insufficient.
4. The position creates tension or pain
Efficient turnout should not rely on constant excessive effort or cause joint discomfort.
How can Clinical Pilates help dancers?
Clinical Pilates does not magically increase the anatomical rotation available at the hip, but it can help dancers make better use of the range they already have.
Through motor control, strength and stability training, Clinical Pilates may contribute to:
- Better pelvic and hip control
- Lumbopelvic stability allows movement to be performed more efficiently, reducing compensations during demanding positions.
- Greater ability to control extreme ranges of motion
- In dance, it is not enough to reach a position: the dancer must be able to sustain it and move within that range with control.
- Improved lower limb alignment
- Strength and neuromuscular control training may help improve the relationship between the hip, knee and foot during functional movements.
- Preparation for the demands of dance
- Clinical Pilates can be integrated into a broader prevention strategy, alongside individual assessment, load management and specific training. Literature highlights the role of Clinical Pilates in conditioning, core control and improving neuromuscular efficiency in dancers.
The key message
In dance, seeking greater range of motion is part of technical development. However, range only becomes an advantage when there is enough control to use it.
Safe turnout is not the one that forces the body to reach a specific position. It is the one that respects the dancer’s individual anatomy and allows movements to be performed with stability, precision and a lower risk of overload.
Before seeking more rotation, it is worth asking:
“Can I control the rotation I already have?”
Learn more about how Clinical Pilates can help you improve your dance performance in this article: Clinical Pilates for Dancers
Find out whether your turnout may be increasing your injury risk: Dance Injury Risk Calculator
At Bwizer Health, we can help you: Dancer Clinical Assessment
References
Critchley, M. L., et al. (2022). Injury epidemiology in pre-professional ballet dancers: A prospective study.
Hrubes, M. (2018). Evaluation and management of the dancer: A clinical approach.
Hrubes, M., & Janowski, A. (2021). Physical therapy evaluation and treatment of dancers.
Junge, A., et al. (2024). Injury patterns and risk factors in professional dancers.
Kenny, S. J., et al. (2018). What are the most common injuries in dancers? A systematic review.
Rinonapoli, G., et al. (2020). Epidemiology and prevention of injuries in dancers.
Van Winden, D. P. J. M., et al. (2019). Musculoskeletal injury and injury prevention in dancers.
Yau, R. K., et al. (2017). Risk factors and injury patterns among dancers.